What is Scapholunate Advanced Collapse (SLAC) Wrist?
Scapholunate advanced collapse (SLAC) wrist is the most common form of degenerative arthritis of the wrist that occurs secondary to traumatic injury of the scapholunate ligament with subsequent collapse on the radial side of the wrist. SLAC wrist is a complication that results due to an undiagnosed or untreated scapholunate interosseous ligament (SLIL) injury, which can often be misdiagnosed as “wrist sprain.” High-intensity contact sports athletes, such as football linemen are specifically susceptible to recurrent SLIL injuries as they undergo high impact and forced wrist dorsiflexion instances for several years in their sporting career.
Anatomy of the Wrist
The wrist is a complex joint that connects the forearm to the hand enabling movement. It consists of 8 small bones called carpals that articulate with two long bones of the forearm (radius and ulna). The scaphoid (at the base of the thumb) and lunate (at the center of the wrist) are carpal bones aligned next to each other and are attached by a ligament called the scapholunate ligament. It is the main stabilizing ligament between scaphoid and lunate bones. The scapholunate ligament consists of 3 well-defined sections: the dorsal, membranous, and volar sections. Although, the volar and membranous sections play a role in the stability of the scapholunate joint, the dorsal section of the scapholunate ligament is the strongest and thickest section, and hence plays the most significant role in stabilization.
Causes of Scapholunate Advanced Collapse (SLAC) Wrist
Even though scapholunate advanced collapse (SLAC) wrist is a commonly experienced progressive type of wrist osteoarthritis that frequently occurs as a result of traumatic injury of the scapholunate ligament, other conditions can also cause SLAC wrist. These conditions include:
- Kienbock’s disease
- Chondrocalcinosis
- Scapholunate non-union advanced collapse (SNAC)
- Idiopathic avascular necrosis of the scaphoid (Preiser disease)
- Midcarpal instability
- Perilunate dislocation
- Intra-articular fractures involving the radioscaphoid or capitolunate joint
Symptoms of Scapholunate Advanced Collapse (SLAC) Wrist
Some of the common symptoms of scapholunate advanced collapse (SLAC) wrist include:
- Difficulty with weight-bearing across the wrist
- Significant pain in the area of the scapholunate interval
- Progressive weakness of the involved hand
- Wrist stiffness
- Weak grip strength
- Tenderness to palpation
- Reduced range of motion of the wrist
Diagnosis of Scapholunate Advanced Collapse (SLAC) Wrist
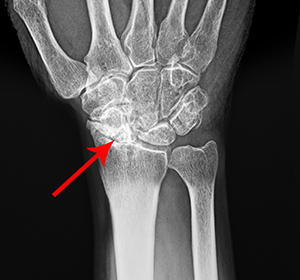
Your doctor will assess your symptoms, take your medical history, and perform a thorough physical examination of your wrist to check for range of motion. Specific diagnostic tests such as Watson scaphoid shift test will be ordered to confirm scapholunate instability. Imaging tests such as X-ray, MRI or CT-scans may be ordered for a detailed evaluation of scapholunate ligament injury and other soft tissue structures surrounding the wrist and to also find out the severity of SLAC wrist in relation to stage I, stage II, or stage III.
Treatment for Scapholunate Advanced Collapse (SLAC) Wrist
The treatment options for scapholunate advanced collapse (SLAC) wrist include nonsurgical methods for mild cases and surgical methods for severe cases. Your doctor will determine the right option for you based on the severity of the condition.
Nonsurgical Treatment
- Activity Modification: Avoiding activities that trigger symptoms and changing one’s habits
- Physical Therapy: Regular exercise regimen to improve range of motion and strengthen wrist muscles
- Anti-inflammatory Medication: Medications like naproxen and ibuprofen to relieve inflammation and pain
- Cortisone Injection: Cortisone is a very effective anti-inflammatory medicine and long-term pain reliever for tears and structural damage.
Surgical Treatment
- SLAC reconstruction (limited wrist fusion): Surgical treatment in the form of wrist ligament reconstruction may be indicated in cases where the wrist ligament is completely torn. The ligament usually will need to be reconstructed when ligament damage is noted after a period of 6 months or more following the initial injury. Ligament reconstruction procedure can be performed as day surgery under local or general anesthesia. During the procedure, your surgeon first makes an incision over your wrist joint to locate the torn ligament. Once located, a tendon graft (tissue obtained from a donor part, usually the palmaris longus tendon of the same wrist) is used to replace the torn ligament. The tendon is harvested through the bottom of your wrist via one or two minor incisions. Your surgeon may then place metal pins to support the repair while healing occurs. The surgical incisions are closed and a dressing is applied.
- Arthroplasty of the wrist: In this procedure, your surgeon removes the affected joint and replaces it with an artificial implant. In patients with post-traumatic arthritis and osteoarthritis where the bone is hard and demand on the hand is moderate, new ceramic implants are used. These are not desirable to use for a severely damaged or unstable joint. In patients with inflammatory arthritis where the bone is not strong enough and the demand on the hand is low, older silicone rubber joints are generally used. These can be used for cases with more severe joint damage and an unstable joint.
- Total wrist arthrodesis: A fusion, also called an arthrodesis, involves removal of the joints and fusing the bones of the joint together using metal wires or screws. Even though this surgery eliminates all motion at the base of the thumb, the resulting fusion is very hard. This surgery is usually indicated when the joints are severely damaged, when there is limited mobility, damage to the surrounding ligaments and tendons, failed previous arthroplasty, and when heavy manual use is expected.
Rehabilitation
Following surgery, the wrist is supported by a splint or cast for 1-2 weeks. You will be instructed on special exercises to regain strength and mobility of your wrist. Complete healing and return to strenuous activities such as sports may take about 6 months.